
NYC Has Retirees’ Best Interests At Heart - So, Where’s The Blue Ribbon Panel On Healthcare?
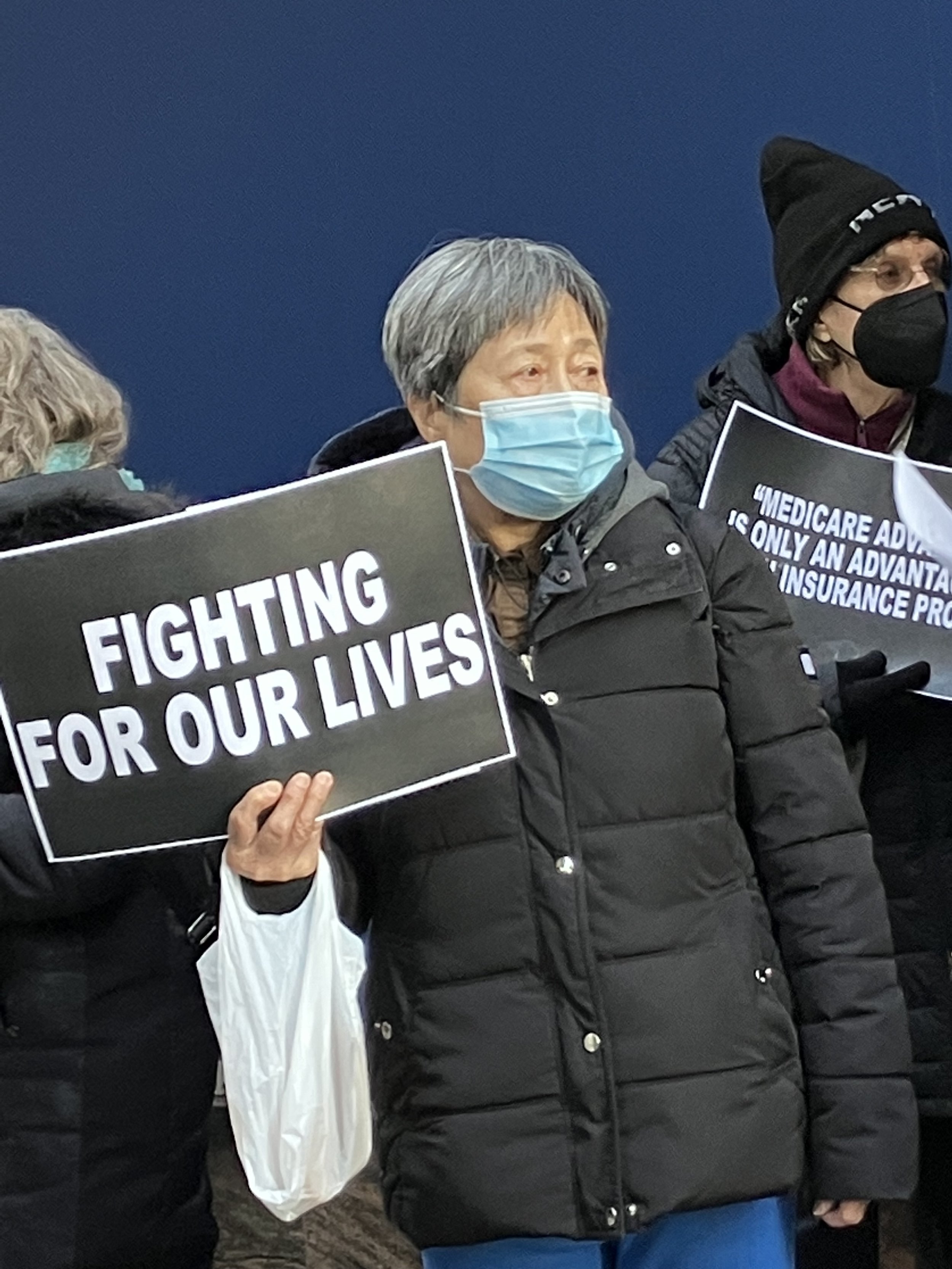
Municipal retirees rally outside UFT offices on Broadway last December against the campaign to push them into privatized Medicare Advantage health insurance. Photo By Joe Maniscalco
By Joe Maniscalco
New York City Mayor Eric Adams, when he announced his support of a plan to push municipal retirees into a privatized Medicare Advantage program last year, said “the city has had, and will continue to have, your best interests at heart.”
Why then does convening a Blue Ribbon Panel where those interests would be directly represented by retirees themselves appear to be the last thing Hizzoner wants to talk about?
Opponents of the campaign to push municipal retirees into a for-profit Medicare Advantage program have long sought a Blue Ribbon Panel that includes retirees and looks for cost-saving measures that preserves their traditional Medicare coverage.
But when Work-Bites reached out to the Mayor’s Office this past week to get the chief executive’s thoughts on the matter — Deputy Press Secretary Jonah Allon declined to address our inquires directly, and instead issued this canned response:
“The administration is committed to offering quality and sustainable care for our retirees. The city and the Municipal Labor Committee worked together to take advantage of the federal funding for Medicare Advantage plans that would permit us to continue providing high-quality, premium free coverage for retirees while saving approximately $600 million a year — savings that are especially critical as we continue to face skyrocketing health care costs and other fiscal challenges. At the recent City Council hearing, we presented a clear case that the city’s Medicare Advantage plan would offer myriad improvements over the current SeniorCare plan, while still encouraging the Council to preserve retiree choice by amending the administrative code.”
Opposition to the campaign to privatize New York City municipal retiree healthcare and push them into a for-profit Medicare Advantage program remains strong amongst retirees and active workers alike — despite the best efforts of the Mayor’s Office and the heads of the Municipal Labor Committee [MLC],
Evidence about just how bad those privatized Medicare Advantage plans really are also remains strong — despite the number of retirees across the country being funneled into them.
Supporters of the privatized plans tout the trendy perks and no-cost premiums they hear from Medicare Advantage barkers. But it’s the delays, denials and prior authorizations associated with privatized Medicare Advantage plans that most concern opponents.
According to the American Medical Association [AMA], prior authorization is a “barrier to providing timely, patient-centered care.”
Indeed, more than 90 percent of those taking part in the AMA’s annual prior authorization physician survey said prior authorizations can lead to “negative clinical outcomes.”
That’s a very sanitized way to characterize the situation — the reality looks a lot grimmer if your own grandmother or some other family member’s well being is involved.
The AMA’s latest survey similarly finds 82 percent of physicians reporting prior authorization can lead to frustrated patients “abandoning their course of treatment.” Another 34 percent say prior authorization has “led to a serious adverse event for a patient in their care.”
And last spring, the U.S. Department of Health and Human Services Office of the Inspector General found Medicare Advantage plans sometimes delayed or denied beneficiaries’ access to services — even though the requests met Medicare coverage rules.
“MAOs also denied payments to providers for some services that met both Medicare coverage rules and MAO billing rules,” the report says. “Denied requests that meet Medicare coverage rules may prevent or delay beneficiaries from receiving medically necessary care and can burden providers.”
The same report further finds that “among the prior authorization requests that Medicare Advantage plans denied — 13 percent met Medicare coverage rules; in other words, these services likely would have been approved for these beneficiaries under original Medicare.”
The Centers for Medicare & Medicaid Services (CMS), meanwhile, have released proposed rule changes attempting to reform the way Medicare Advantage plans operate.
This is just a small sampling of the reasons why retirees want real alternatives to Medicare Advantage — and a Blue Ribbon Panel on the future of not only their healthcare — but all of the municipal retirees following them.
What they’ve gotten instead, however, are a lot of vague assurances from the heads of the MLC and the Mayor’s Office saying things like they’ve “eliminated a lot of the pre-authorizations already.”
That’s also what municipal retirees in Delaware were told before they learned the Medicare Advantage contract being foisted on them contained over 2,000 prior authorizations involving both medications and medical procedures.
UFT President Michael Mulgrew told Gothamist “New York City can create a unique Medicare Advantage plan, provided we find the right partner.”
“How will they know that the ‘unique to NYC’ program is actually a viable program for the needs of unique NYC retirees without a science-based study?” municipal retiree Roberta Gonzalez tells Work-Bites. “How will they determine what’s unique to NYC retirees? Standards? Measures? Evaluations? Where is the science? If there’s no science — it’s a ploy. They’re giving big bucks to private industry insurance salesmen who have no interest except to make money by delaying and denying care.”
The city maintains it needs to close a $600 million budgetary gap and that’s why it wants to grab those federal dollars and push retirees into a privatized Medicare Advantage program. Opponents have already gone to great lengths to offer viable alternatives, however.
Stuart Eber, president of the Council of Municipal Retiree Organizations, as well as president emeritus of the NYC Managerial Employees Association says the veracity of that $600 million figure itself needs further scrutiny.
“That $600 million number, at this point, needs to be revised,” Eber tells Work-Bites. “And part of what this [Blue Ribbon Panel] would have to do is really dig down into the numbers. In 2018, when all this started, there were 327,000 employees. Now, there’s 301,000. That’s a reduction of roughly seven percent. The total cost of healthcare per year, supposedly, is $10 billion. Seven percent of $10 billion is $700 million. So, theoretically, that’s $700,000 less the city is spending now.”
Eber stresses the need for the Independent Budget Office and Comptroller to “cross reference and verify” the figures “so that we all know actually how much money needs to be saved.”
“Different groups have come up with a variety of suggestions, particularly the Professional Staff Congress, on how to save hundreds of millions of dollars,” Eber adds. “That’s why you need an independent group that has all the stakeholders at the table to do this the right way and not having to revisit this every three to five years.”
The heads of the MLC like to point out that the Medicare Advantage plan they are attempting to concoct would be based on a PPO model rather than a narrower HMO model.
Eber, however, calls that “the lesser of two evils” — one that still involves a “complicated mechanism for reimbursements.”
“As opposed to traditional Medicare where there isn’t anything in between — it’s just you and the provider, and the provider sends the bill to Medicare and Medicare reimburses pays them. Plain and simple,” Eber says.
Gonzalez, who helped New York City clean up in the immediate aftermath of 9/11 and is now battling cancer, PTSD and depression, says city retirees want excellent healthcare — not “silver sneakers, meals-in-a-box or any other gimmick.”
“We put our lives and health at risk working in old, dilapidated city buildings with lead, asbestos and other toxins,” the Brooklyn retiree says. “Firemen walk into burning buildings and breathe in god knows what; Police and Sanitation folks are at risk; Health Department folks have had needle sticks when HIV was new; Clinic staff are at risk for active and latent TB. These jobs keep the city running, so that the folks who don’t have to do these jobs hardly ever think about the things that go into making the city run, until there’s a breakdown.”
The heads of the MLC, of course, argue that under the Taylor Law unions can only represent those in active civil service. Eber says he doesn’t have a problem with that.
“That doesn’t give them license to sell out the retirees,” he says. “The commitment to us was when you retire you will have your Medicare and the city will provide the supplemental — period. And now they’re trying to undue that.”